
The original SARS-CoV-2 virus was responsible for the the large first wave of hospitalizations and deaths that overwhelmed an unprepared world. Most deaths were in the elderly who were inadequately protected.
In the absence of easy effective containment measures and vaccines, lockdowns were used in most countries to slow the spread of disease. In this initial wave, COVID-19 mortality was mainly a disease of the elderly or the unhealthy.
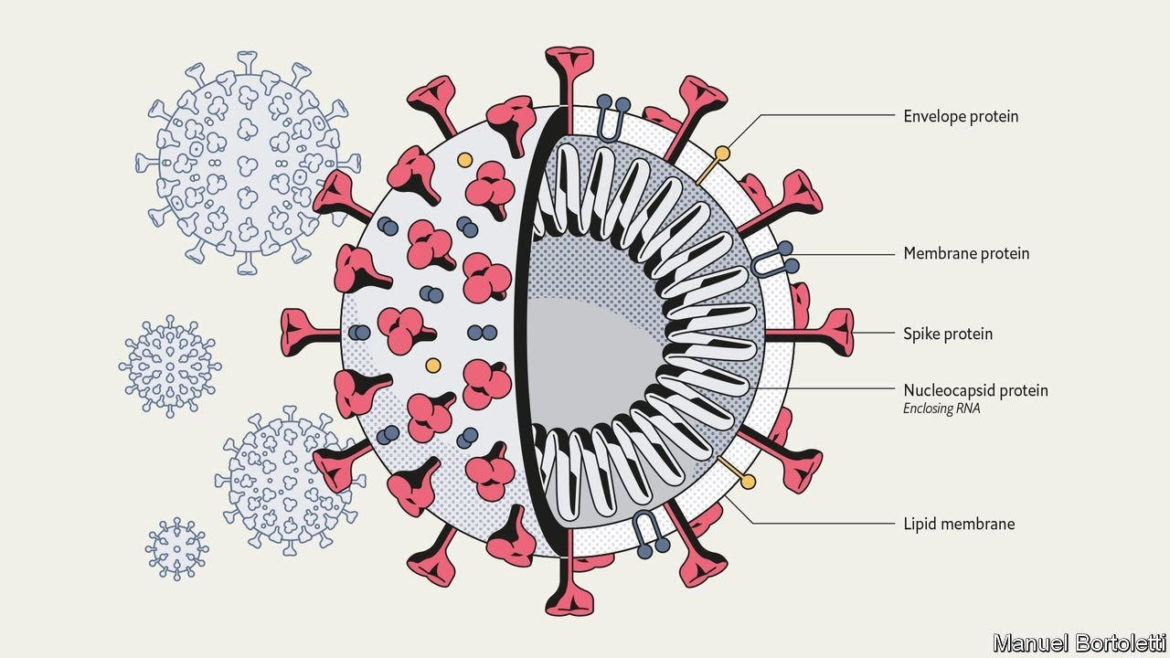
The virus is made up of various components and proteins as shown below. The spike protein is the most important since it is the entry point for infiltrating cells and then using the cell’s machinery to extensively replicate and spread.
As time went on and infection rates increased, the viral replication was sometimes imperfect leading to a mutation, that is an alteration in the genetic code resulting in a change in the virus’ protein.
While some of these mutations occurred in all the viral protein components and were often harmless, they were most threatening when they occurred in the spike protein because disease burden increased as the mutation allowed easier entry into cells.
Variants of interest and concern
Mutations occurring in the virus were monitored by genetic sequencing of the viral proteins. Those not highly prevalent or more dangerous were called variants of interest and monitored.
When the viral mutations were shown to be more contagious and caused more severe disease burden they were upgraded from being called variants of interest to being labelled variants of concern (VOC).
These VOCs were first recognized in the U.K., South Africa, Brazil and finally India and were renamed by the WHO with Greek letters Alpha through Delta. The Lambda variant which originated in Peru is not widespread yet in most regions and thus remains a variant of interest.
Why is the Delta variant concerning?
The Delta VOC is now dominating new infections in much of the world and is spreading 50 percent faster than the originally worrisome Alpha variant which itself spread 50 percent faster than the original wild type virus.
Eric Topol, a noted cardiologist and COVID expert has said that the increased risk is due to the virus replicating faster with a shorter incubation period leading to a higher viral load in an infected person.
COVID-19 disease burden relates to the viral load a person is exposed to, which in part explains the greater risk of infection with a VOC that generates higher loads because it replicates faster. Thus the Delta variant is much more transmissible with larger amounts of airborne virus and leads to more super-spreader events and higher numbers of infected people.
So while it is not clear that the Delta variant is much more virulent and deadly by itself, it is more deadly because it creates more cases of disease and thus overall higher numbers of hospitalizations and deaths.
The Delta variant is now dominating new infections in most parts of the world. It is now the cause of over 85 percent of infections in the U.S.
While with the original wild type virus very few young healthy people were being hospitalized or dying, we have now seen a major increase in this population who are no longer relatively safe without vaccination.
The impact of infection on death
As of July 27 The Public Health Agency of Canada reported over 1.4 million cumulative infections and 26,553 deaths.
These deaths represent about 0.1 percent of our overall population or a rate of about 700 per million population. The overall calculated death rate if infected is about 1.9 percent and is heavily skewed to the elderly and those with co-morbidities.
The death rate is likely lower, perhaps 1-1.5 percent since many low grade or sub-clinical infections were not counted especially when testing was not routinely done. While the percentage of the population dying seems low, the deaths that occurred were individual tragedies and more so since so many were preventable deaths.
Hospitalization and ICU care
The disease burden is of course greater than simply the number of deaths.
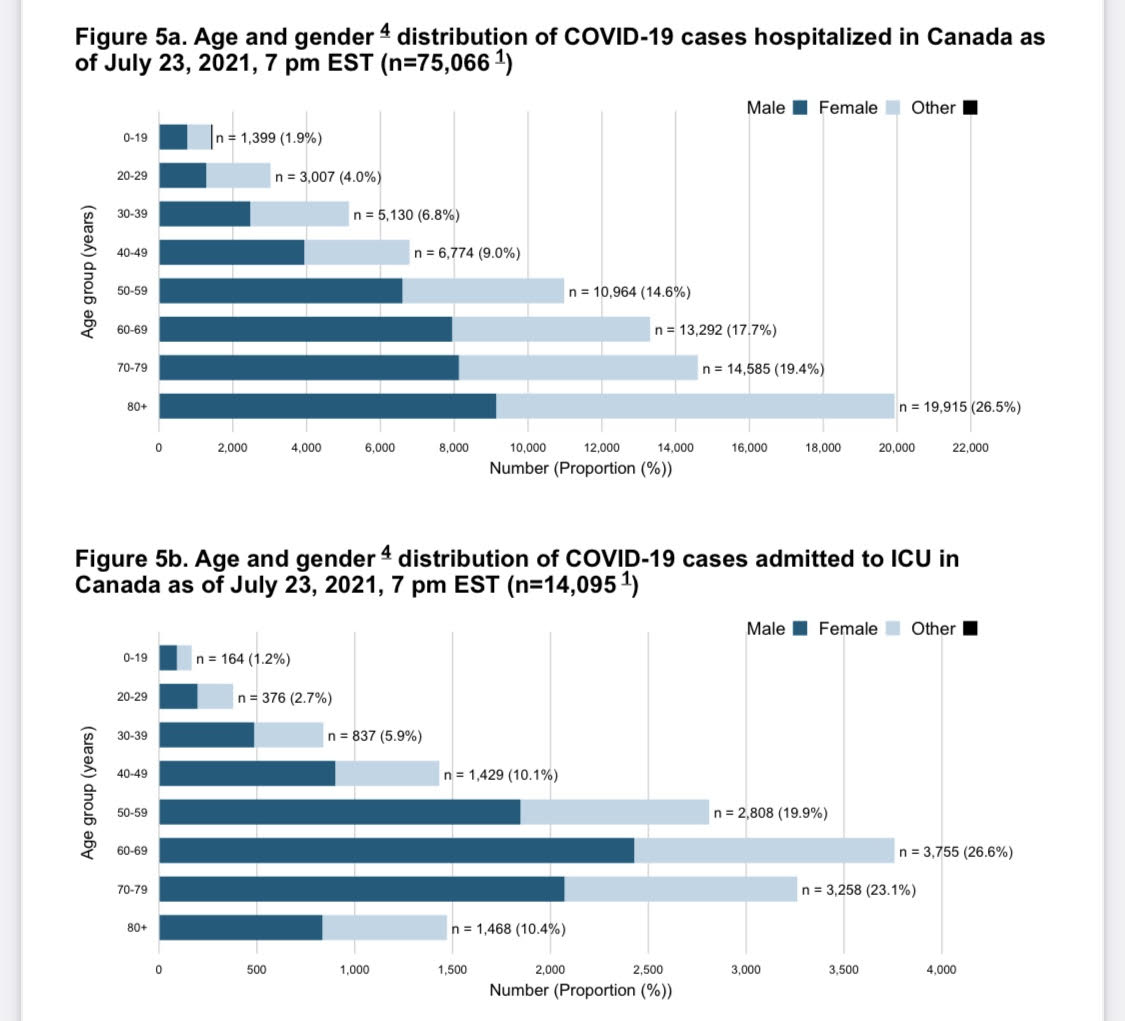
The hospitalization rate is about 7.5 percent of infections, of which 19 percent of those hospitalized require ICU care and 2.6 percent mechanical ventilation. The age and gender distribution of hospitalized and ICU cases is shown below.
The disease is not benign even for those under 40. This age group accounted for 12.7 percent of hospitalizations and 9.8 percent of ICU admissions. This percentage continues to increase as older people are highly vaccinated and protected and younger people are more vaccine hesitant.
Those that survive are often left with lingering illness and emotional trauma after their brush with death.
Vaccine hesitancy and individual risk
Vaccine hesitancy remains higher in younger people often because they believe their risk of hospitalization and death is very low. The higher viral loads with the Delta VOC have led to more symptomatic and life threatening infections. Anyone hospitalized and fearing ventilation and death typically regret their choice to not be vaccinated.
The low mortality rate should also not be too comforting for the young when you realize the possible misery of being seriously ill, hospitalized and dying badly. The lingering effects of long COVID can also be debilitating. The risks of becoming infected simply put remain much higher than the low risks of vaccination.
Restrictions will ease for the vaccinated and increase for those who choose to remain unvaccinated.
Countries such as Canada, U.K. the U.S. and Israel have very high rates of full vaccination especially in their older population who are thus relatively protected from bad outcomes even from the Delta variant. The disease is becoming primarily a disease of the unvaccinated and those older people whose vaccine immunity is pierced.
After a truly dysfunctional vaccine procurement and roll out, Canada now is at the forefront of rates of full vaccination. Vaccine boosters will soon likely be available to further protect the most vulnerable when the Delta variant increasingly pierces immunity as it is starting to do. We need carefully collected data to inform us when and in whom boosters are required.
The rest of the world is starting to catch up on vaccination rates. According to Our World in Data globally about 4 billion vaccine doses have been administered increasing by 34 million shots daily. We need to continue to help poorer countries by providing vaccines and essential medicines including oxygen.
While the Delta variant likely increases the vaccination levels needed for herd immunity, we are getting closer in Canada. Restrictions will ease for the vaccinated and increase for those who choose to remain unvaccinated.
We need to continue to be vigilant but focus on how to restart life, learn from the hard lessons of what we did wrong, protect jobs and grow our economy. Hardship and restrictions make you value freedom and safety more than ever.
Recommended for You

‘Not a guide to practical action’: David Frum on 60 years of George Grant’s Lament for a Nation

Ginny Roth and Brian Dijkema: Why Ontario should allow independent schools and unlock true choice in education

Need to Know: Canadian multiculturalism is ‘dangerously adrift’

Falice Chin: A tale of two (Poilievre) ridings

